The Fundamental Question
How does investing in 1,825 Black queer men receiving therapy over 5 years transform mental health attitudes across 35,000 Black queer men in the UK? How do spoke city events in Manchester and Birmingham create cultural shifts in London, Leeds, Bristol? How does a cohort of 10 specialists embedded in institutions change national policy?
The answer lies in network effects: behaviours and beliefs spread through social networks in predictable, measurable ways. Individual interventions become collective transformation when they reach critical mass within the right network structures.
Network Effects: The Science of Cultural Change
What are network effects? When the value/impact of a behaviour increases as more people adopt it. One person in therapy = individual healing. 365 people in therapy annually = normalization. 1,825 over 5 years with visible results = cultural shift where "therapy is for us too."
Why they matter for mental health: Mental health stigma persists not because individuals lack information, but because social networks reinforce silence. When Black queer men see others in their community accessing therapy, talking about mental health, thriving through support—the network effect reduces stigma faster than any public health campaign.
The power of "small world" networks: Black queer communities already have dense local connections (friendship groups, club nights, social scenes) with some long-distance ties (people who moved to Manchester, Birmingham, Bristol from London). This structure enables rapid diffusion: innovations spread locally through dense clusters, then jump across geography through long-distance ties, reaching the entire network faster than hierarchical or random networks.
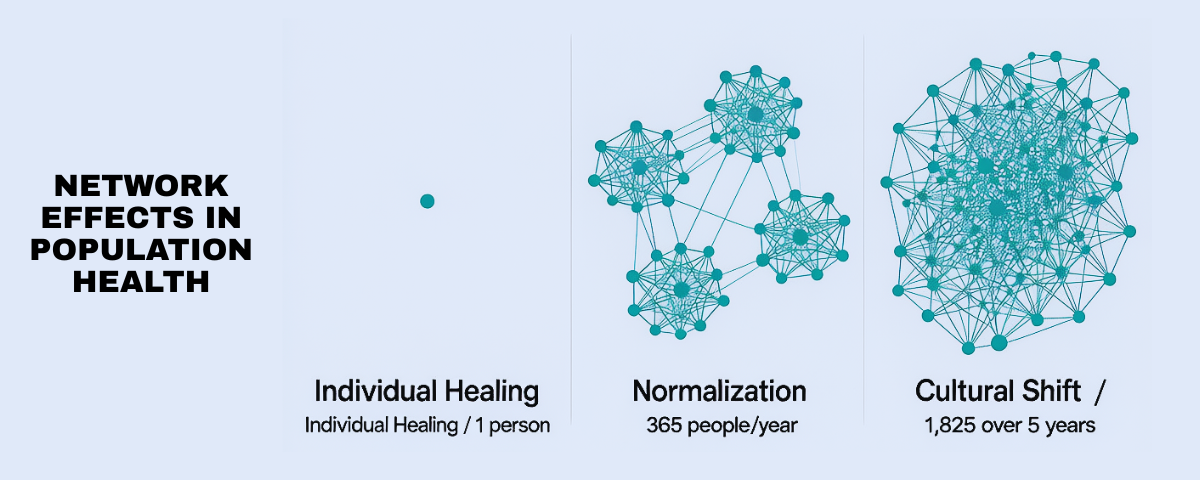
Network effects in action: From individual healing (1 person) → normalization (365/year) → cultural shift (1,825 over 5 years)
Mechanism 1: Complex Contagion & Critical Mass
Simple vs. Complex Contagion (Centola 2018)
Simple contagion: Spreading information or disease—one exposure sufficient. "Did you hear about the new club night?" spreads through single contacts.
Complex contagion: Spreading behaviours requiring social reinforcement—multiple exposures from multiple sources needed. "I'm going to therapy" spreads when you see several trusted peers doing it, not just hearing about it once.
Mental health behaviours = complex contagion. Deciding to access therapy, talking openly about mental health struggles, accepting help—these require social proof from multiple sources. One friend in therapy might be "unusual." Three friends in therapy suggests "this is something people like me do."
Critical Mass: The Tipping Point for Therapy Normalization
The numbers: 365 Black queer men/year receiving therapy × 5 years = 1,825 individuals. Population = 35,000. That's 5.2% direct intervention rate.
Why 5.2% creates system-wide change: Research on complex contagion shows tipping points between 15-25% of a network needed for new behaviours to become self-sustaining. But here's the crucial insight: those percentages refer to people exposed to the behaviour, not the total population.
Network amplification: Each person in therapy is connected to approximately 20-30 close ties (friends, family, partners, community members). 1,825 people × 25 average connections = 45,625 exposure points. That's 130% of the total population—meaning most Black queer men will know multiple people who've accessed therapy through this programme.
Multiple exposure = behaviour change: When someone knows 3-4 people in therapy (not just one), the behaviour shifts from "unusual" to "normal." Network structure ensures most people will have multiple exposures, crossing the threshold for complex contagion.
Mechanism 2: Hub-and-Spoke as Small World Network
Why Geography Matters for Network Effects
The problem: 60% of Black queer men live outside London. If interventions only reach London, network effects stay localized—Manchester doesn't benefit from London's cultural shifts, Birmingham remains isolated.
Small world solution: Hub-and-spoke infrastructure (London centre + Manchester/Birmingham/Bristol events) creates the optimal network structure for rapid diffusion. Dense local clusters (London scene, Manchester scene) connected by "long-distance ties" (people who moved, people who travel, people with friends in other cities).
How diffusion works: Therapy normalization starts in London cluster (high density of programme participants). Spreads locally through dense connections. Then jumps to Manchester through long-distance ties. Spreads locally in Manchester. Jumps back to London + Birmingham. Entire network saturated faster than if concentrating only on London.
The mathematics (Watts & Strogatz 1998): Small world networks reduce average path length between any two nodes from O(n) to O(log n). Practical meaning: behaviour spreads exponentially faster. Instead of reaching 35,000 people in linear sequence (years), reaches them in logarithmic sequence (months).
Spoke City Events as Diffusion Accelerators
What the investment buys: Regular events in Manchester, Birmingham, + spoke cities where people develop interests, share experiences. Group travel subsidies connecting hub-spoke-community. Not just "services outside London" but deliberate network architecture.
Network effect mechanism: Events create temporary high-density clusters where multiple people in therapy interact with multiple people not yet in therapy. Creates the "multiple exposure" conditions necessary for complex contagion. Someone attends Manchester event, meets 4 people who've benefited from therapy, social proof threshold crossed.
Community media as accountability infrastructure: Not peripheral "arts programming" but core mechanism for monitoring and communication. Community-produced media (podcasts, videos, newsletters, social content) creates ongoing documentation of specialists' work, institutional changes, therapy experiences. Enables community to hold institutions accountable in real-time, not waiting for annual reports.
Bypassing legacy gatekeepers: Direct communication with community without mainstream media filtering/distortion. When specialists document institutional racism, community media publishes it immediately. When therapy helps someone, they share testimony directly. When institutions resist reform, community knows without PR spin. Network effects amplified because information spreads through trusted community channels, not legacy media that historically misrepresents Black queer experiences.
Dancing, arts as strong tie formation: Creating together, performing together, celebrating together = strong tie formation. Strong ties = trusted sources for complex contagion. Weak ties (acquaintances) spread information; strong ties (friends, chosen family) spread behaviour change. Arts/dancing not separate from media—they're content creation, documentation, cultural production strengthening network bonds.
Measurable outcome: By Year 3, expect to see therapy uptake rates higher in spoke cities than statistical distribution would predict—evidence of network diffusion, not just individual access.
Tipping Points: When Individual Becomes Collective
Year 1-2: Early Adopters & Local Clustering
Individual: 730 Black queer men access therapy, start talking about mental health, visible in community.
Network: Early adopters cluster in dense social networks (London scenes, Manchester communities). Their close ties begin receiving multiple exposures. Stigma reduction within these clusters.
Tipping point status: 2% direct intervention, approximately 10-15% network exposure. Below critical mass for system-wide change, but building foundation.
Year 3: Critical Mass & Diffusion Acceleration
Individual: 1,095 total men accessed therapy. Cohort of 10 specialists visibly embedded in institutions, reporting changes.
Network: Multiple exposures reach threshold. "I know several people in therapy" becomes common. Behaviour shifts from unusual to increasingly normal in dense clusters. Long-distance ties carry behaviour to spoke cities. Media/arts/dancing interventions strengthen ties, accelerating diffusion.
Tipping point status: 3.1% direct intervention, approximately 20-25% network exposure. Approaching critical mass in some clusters, behaviour becoming self-sustaining.
Year 4-5: Self-Sustaining Cultural Change
Individual: 1,825 total men accessed therapy. Specialists documenting institutional changes. Infrastructure decisions made democratically for Years 6-10.
Network: Tipping point crossed in multiple clusters. Therapy normalization self-sustaining—people accessing therapy without direct programme contact because "everyone's doing it." Spoke cities show independent uptake. Cultural narrative shifts: mental health support becomes "part of Black queer community care."
Tipping point status: 5.2% direct intervention, 30-40% network exposure through multiple contacts. Behavior normalized, spreading beyond programme participants.
Years 6-10: Institutionalized Cultural Norms
Individual: Programme participants now community leaders, therapists, institutional change agents. New cohorts entering therapy without stigma.
Network: Cultural norm fully institutionalized. Community-owned infrastructure (from development lab) sustaining support. Cohort of specialists now senior leaders, training next generation. Mental health literacy embedded in community culture.
Tipping point status: Irreversible cultural change. Network effects creating compounding returns beyond initial investment.
Mechanism 3: Institutional Embedding & Structural Change
How 10 Specialists Change National Policy
Traditional advocacy model: External pressure on institutions. Institutions resist, make cosmetic changes, revert when pressure subsides. No lasting network effects.
Embedded cohort model: Specialists inside institutions create internal advocacy networks. Build relationships with decision-makers. Demonstrate what works. Reform spreads through institutional networks (NHS trusts talk to each other, housing associations share practices).
Network diffusion across institutions: Specialist in NHS Manchester reforms mental health pathway. NHS Birmingham hears about it through professional networks. Adopts similar approach. NHS Leeds invites specialist to consult. Innovation spreads through institutional network, reaching far beyond 10 host organisations.
Two-way network effects: Specialists gain institutional reform skills, become sector leaders. Their career progression carries community knowledge into new organisations. One specialist moves from housing association to national policy role—entire network of housing providers now accessible for reform. Compounding returns through career mobility.
Measurable outcome: By Year 5, expect to see policy changes in organisations with no direct programme contact—evidence of institutional network diffusion.
Community Media as Accountability & Amplification Network
Traditional accountability problem: Institutions publish annual reports months after decisions made. Community learns about failures/successes through legacy media filtering Black queer perspectives. No real-time accountability, no community voice in narrative.
Community media solution: Ongoing monitoring through community-produced content. Specialists document institutional barriers/breakthroughs in real-time. Community members share therapy experiences, mental health journeys, cultural shifts through podcasts, videos, newsletters, social media. Democratic governance holds specialists accountable through transparent reporting.
Network effect mechanism: Community media creates multiple exposure points for behaviour change. Someone hears podcast episode about therapy experience (exposure 1). Sees video of specialist discussing NHS reform (exposure 2). Reads newsletter about community member's healing journey (exposure 3). Multiple exposures from trusted sources = threshold for complex contagion crossed.
Bypassing legacy gatekeepers: Direct communication with community without mainstream media distortion. When specialist documents institutional racism, community media publishes immediately—institutions can't control narrative. When therapy normalization succeeds, community tells story in own voice. Legacy media historically misrepresents/sensationalizes Black queer experiences; community media ensures authentic representation spreading through trusted networks.
Amplification through legacy networks: Community media doesn't ignore legacy media—it changes power dynamic. Instead of community waiting for Guardian/BBC to cover mental health story (with inevitable distortion), community produces evidence-based content legacy media must reference. Specialists become expert sources journalists contact. Community controls narrative entering legacy networks, ensuring accurate representation reaching wider audiences.
Measurable outcome: By Year 3, expect community media content referenced by legacy media outlets, specialists quoted as experts, community narrative shaping national mental health discourse—evidence of network amplification beyond community boundaries.
Why Network Effects Justify the Investment
The ROI of Cultural Change
Direct impact: 1,825 individuals receiving therapy. 10 specialists reforming institutions. Hub-and-spoke infrastructure connecting community.
Network-amplified impact: 45,625 exposure points creating multiple contacts for most Black queer men. Therapy normalization reaching beyond direct participants. Spoke cities showing independent uptake. Institutional reforms spreading to organisations without embedded specialists.
Why traditional programmes fail: They don't account for network effects. Provide services to individuals, measure individual outcomes, miss the collective transformation. Therapy uptake stays at 3.8% because social networks still reinforce stigma.
Why this programme succeeds: Deliberately engineers network effects. Creates critical mass for complex contagion. Builds small world network architecture for rapid diffusion. Embeds specialists in institutional networks for structural change. Measures not just individual healing but cultural transformation.
The compounding return: Year 1 investment creates Year 2 network effects which create Year 3 tipping points which create Years 6-10 self-sustaining cultural change. £10.5M investment buys perpetual return through institutionalized cultural norms.
Evidence Base: Network Effects in Practice
Empirical Support (Centola 2018, 2021)
- Health behaviour adoption: Complex contagion studies show behaviours requiring social proof (exercise, diet change, medical screening) spread through networks with 15-25% thresholds. Obesity, smoking cessation, happiness all show network diffusion patterns.
- Small world networks: Watts & Strogatz (1998) demonstrated small world structure reduces diffusion time exponentially. Empirically validated across biological, social, technological networks.
- Tipping points for social change: Centola et al. (2018) demonstrated 25% committed minority sufficient to tip majority to new norm. But crucially: those 25% must be distributed across network, not clustered in isolated groups. Hub-and-spoke ensures distribution.
- Institutional network diffusion: Policy innovations spread through professional networks (Mintrom 1997). Successful pilot programs adopted by peer organisations through network contacts, not top-down mandates.
Application to Black Queer Mental Health
Why existing interventions fail network test: Individual therapy provision without community context. No critical mass for complex contagion. No small world architecture for rapid diffusion. No institutional embedding for structural change. Network effects work against intervention (stigma reinforced).
Why this intervention passes network test: Creates critical mass (1,825/35,000 = 5.2% direct, 130% network exposure). Builds small world structure (hub-and-spoke). Embeds in institutional networks (10 specialists). Strengthens ties through media/arts/dancing. Network effects work for intervention (normalization reinforced).
Predicted outcomes if network theory correct:
- Year 3: Therapy uptake rates exceed statistical predictions in spoke cities (evidence of diffusion)
- Year 4: Self-reported stigma reduction in people with NO direct programme contact (evidence of network effects)
- Year 5: Institutional policy changes in organisations WITHOUT embedded specialists (evidence of institutional diffusion)
- Years 6-10: Sustained cultural change requiring no ongoing programme funding (evidence of tipping point crossed)
Conclusion: From Individual to Collective
The £10.5M cohort leadership investment buys more than 1,825 individuals in therapy, 10 specialists in institutions, hub-and-spoke infrastructure. It buys the network conditions for individual interventions to become collective transformation.
365 men/year in therapy is not a service delivery number—it's a critical mass calculation for complex contagion.
Hub-and-spoke infrastructure is not geographic equity—it's small world network architecture for exponential diffusion.
10 embedded specialists is not institutional partnership—it's network infiltration for structural change spreading through professional ties.
Community media is not peripheral programming—it's the accountability infrastructure enabling democratic governance, the communication channel bypassing legacy gatekeepers, the content creation strengthening network ties through shared cultural production.
Network effects transform individual healing into collective cultural change. Individual therapy becomes community normalization. Individual specialists become sector-wide reform. Individual spaces become national movement infrastructure.
Without community, there is no liberation—not because individuals need community support (though they do), but because liberation IS the network effect where individual transformation becomes collective power, where isolated healing becomes cultural shift, where 1,825 people accessing therapy becomes 35,000 people living in a community where mental health support is normal, expected, celebrated.
That's the outcome network effects predict. That's the return this investment will deliver.