Introduction
A government elected promising change has finally updated the Mental Health Act after 40 years. Lord Darzi has set the direction. The 10-year plan published in July states: "Our reimagined NHS will be designed to tackle inequalities in both access and outcomes... This is a plan to transform the NHS into an engine for economic growth: hospital to community, analogue to digital, sickness to prevention." The Inquiry into LGBT Health Inequalities reports by the end of this year.
Black-led civil society organisations are more focused on mental health and innovating in policy, practice and advocacy. We are proud to work in solidarity with so many through the Black Mental Health Manifesto.
This briefing presents an account in three senses: describing the reality of community-led mental health innovation, counting the real costs of current failures and future solutions, and establishing accountability frameworks that enable genuine partnership between communities and institutions. Black queer men in the UK have developed working interventions that deliver better outcomes at lower costs. The question is whether institutions will invest in scaling what works.
Why Now? The Window of Opportunity
Systems tried to force us into silence and shame, isolating us from each other and from communities we needed for support, requiring us to choose sides and trust no one—ourselves included. We live (and die) with the repercussions. Our survival is a triumph.
Now, in a moment where it is evident that the only constant is change, we have unprecedented opportunity to achieve transformative change in the life chances of Black queer men in the UK. Seeking merely to stand still, to survive in the midst of new possibilities betrays the legacy of struggle that typifies our history. Like poet Essex Hemphill, we too 'want to start an organisation to save our lives'. Digital technology offers new possibilities alongside great threats. An economy where inequality is the only metric that consistently grows. Global alliances, like global temperatures, are moving erratically, creating unexpected consequences for all whilst reserving especially dire outcomes for the poor and powerless.
This is the historical moment where Black queer men's survival innovations become blueprints for transformation. Where our forced expertise in navigating hostile systems reveals how to build better ones. Where our refusal to disappear becomes the foundation for collective thriving.
The Opportunity Before Us
From Greenwich to Glasgow, Bradford to Brixton, Swansea to Sunderland, Black queer men are "forging solutions in the crucible of difference" (Audre Lorde). With limited resources and against considerable odds, communities are demonstrating what genuine mental health support looks like when it centres those most affected.
The evidence is clear: NHS services are failing Black communities. Peer-led interventions demonstrate promise in addressing isolation and building community connection, though rigorous outcome data for Black queer populations specifically requires further research investment. These aren't experimental programmes—they're working interventions happening now, doing what we can from where we are, with what we have.
The question before decision-makers is not whether to invest in untested ideas. It's whether to scale what's already working or continue with systems that deliver high spending and low returns.
Account: Describing the Reality
What Community Wisdom Already Knows
Black queer men in the UK face intersecting pressures that mainstream mental health services were never designed to address. Colonial violence didn't end with empire—it evolved into systems that pathologise difference, criminalise survival, and medicalise resistance.
NHS talking therapies achieve 50-60% success rates for depression and anxiety in general populations, but when services don't understand how racism, homophobia, and economic marginalisation compound, they can't heal what they can't see.
Communities responded by building what was needed. Peer support networks that understand lived experience. Cultural spaces where African and Caribbean spiritual practices aren't dismissed as superstition. Social platforms free from the racism endemic to mainstream gay dating apps. Mutual aid systems that recognise financial precarity as trauma, not personal failure.
"These aren't supplements to 'real' mental health care—they're interventions that address root causes NHS services ignore."
The evidence validates community wisdom. The current approach is the expensive option—it just distributes costs across emergency services, criminal justice, and bereaved communities rather than investing in prevention.
The Master's Tools Cannot Dismantle the Master's House
As Audre Lorde taught, those forged in the crucibles of difference develop survival skills that academic institutions cannot teach. Black queer men navigating NHS mental health services encounter systems that may offer evidence-based interventions whilst remaining structurally racist and homophobic.
A cognitive behavioural therapy protocol can be perfectly administered whilst failing to address that a client's anxiety stems from immigration enforcement, police harassment, or family rejection. Community-led approaches don't just add cultural competency to existing services—they rebuild from foundations that centre intersectional experience.
This isn't exceptional practice that applies only to marginalised communities. The innovations emerging from margins reveal failures in how public services engage all citizens. When Black queer men demonstrate that peer support outperforms professionalised services, the lesson isn't "special provision for special groups." It's that public services designed in partnership with those affected deliver better outcomes than services designed for populations by institutions.
Account: Counting the Real Costs
What We Currently Pay for Failure
Mental health crisis among Black queer men isn't natural or inevitable—it's produced by systems that could choose differently. The current annual costs are substantial:
NHS provision offers treatments that achieve 50-60% success rates whilst leaving structural causes unaddressed. Emergency mental health services respond to crises that community-led early intervention could prevent. Each psychiatric admission costs thousands; each suicide attempt requiring intensive care costs £1.67 million. These aren't investments in health—they're expenditure on managing failure.
Lost economic contribution mounts when talented, capable people cannot participate fully in society because systems meant to support them instead harm them. Suicide costs £3.12 million per person in direct and indirect impacts. Chronic mental health conditions that keep people from employment, education, and community participation represent capabilities the UK cannot afford to waste.
Community capacity exhausted through unpaid labour represents perhaps the largest hidden cost. Black queer men currently provide peer support, crisis intervention, cultural reclamation, and social infrastructure without compensation or institutional recognition. This isn't volunteerism—it's survival work communities shouldn't have to self-fund whilst paying taxes for services that fail them.
What It Costs to Work at Community Scale
The UN reparations framework identifies five elements: restitution, compensation, rehabilitation, satisfaction, and guarantees of non-repetition. This investment responds to each violated principle with specific interventions. For detailed cost breakdown, see the accompanying Cost Model paper.
Responding to Isolation: Career Fellowship Programme
Black workers in mental health and social care sectors report isolation, workplace victimisation, and watching their efforts fail to change outcomes. This investment creates a cohort leadership fellowship—comparable to Civil Service Fast Track or Clore Leadership—enabling Black queer men to gain cross-sector experience whilst protected from tokenisation.
The fellowship model: Specialists cycle through 18-24 month placements across NHS mental health trusts, housing associations, social care, legal advocacy, arts/culture, and employment/education sectors. A consultancy team champions fellows (not managing them), coordinates cohort learning, synthesises cross-sector insights, and protects from institutional victimisation. Fellows gain institutional reform expertise; partner organisations gain tools to limit the power of racism and homophobia in their systems through two-way learning. By Year 5, fellows transition to permanent senior roles, with some cycling into consultancy team positions to champion the next cohort.
Partnership expectations: Host organisations contribute supervision, workspace, professional development infrastructure, and pathways to permanent roles. The investment covers fellows' salaries, partnership overhead ensuring proper support, and consultancy team advocacy. This isn't "free staff"—it's co-investment in sector transformation where organisations demonstrate commitment through integration, not just hosting.
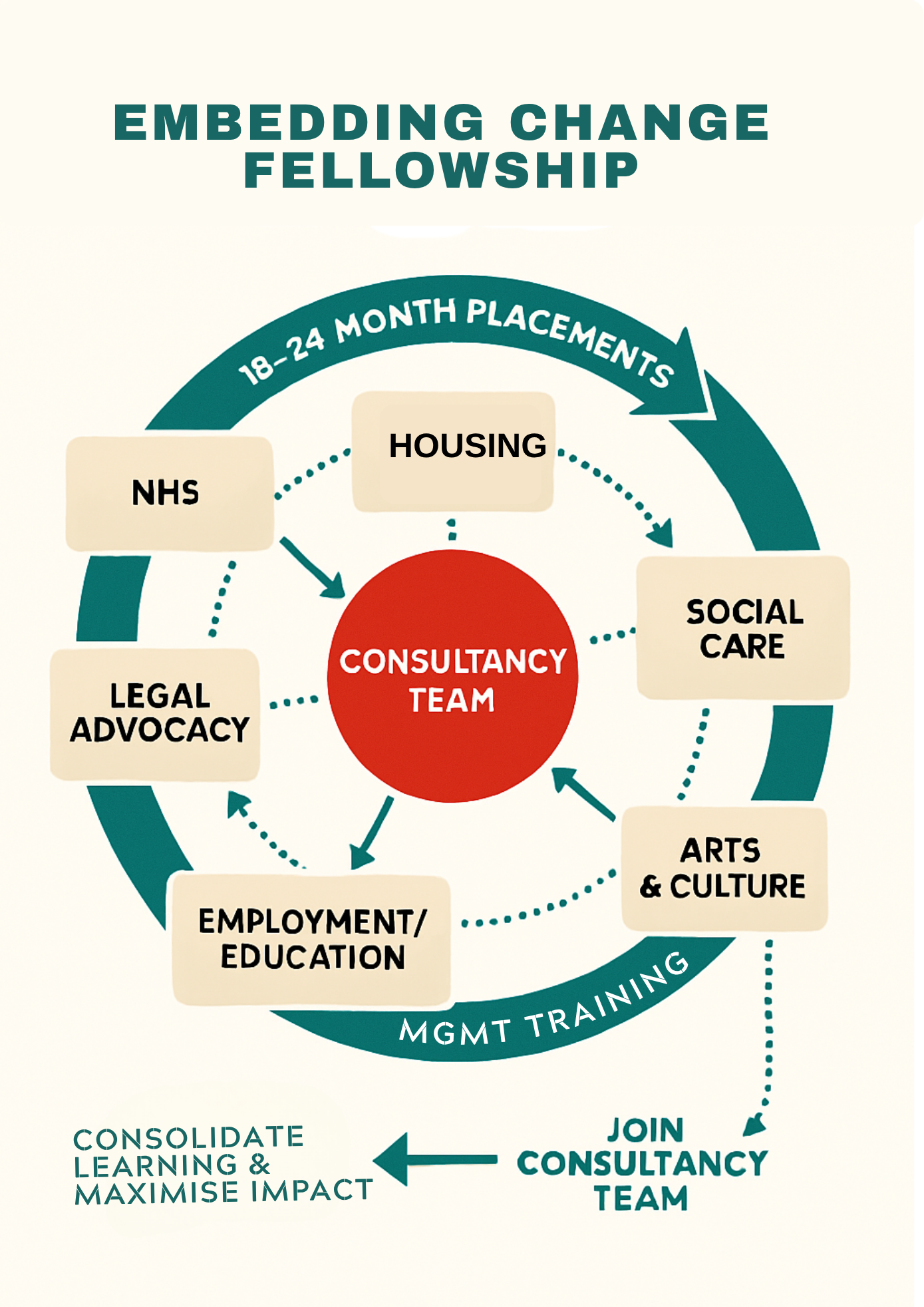
Fellowship model: Specialists cycle through 18-24 month placements across sectors, championed by consultancy team, with pathways to senior roles or consultancy positions
Responding to Service Gaps: Community-Directed Resources
Cultural strategy addresses therapy stigma (3.8% NHS completion rate for Black groups) and geographic isolation (22% loneliness vs 9% general population). Therapy normalization: 365 men/year accessing culturally competent care, building cadre of Black queer therapists. Hub-and-spoke infrastructure: London centre connecting to Manchester, Birmingham, spoke cities where people develop interests, share experiences through media, arts, dancing interventions creating joy and connection. Travel experiences with group subsidies connecting hub-spoke-community, enabling face-to-face relationships across geographic isolation.
Digital courses and self-organising support: Platform enables members to develop skills, share knowledge, and coordinate mutual aid without waiting for institutional permission. On joining, members receive a welcome pack including a bespoke journal designed for Black queer men's reflection and growth, plus access to an accountability partner—peer support relationships that sustain commitment to wellbeing goals without institutional oversight. Marketplace for goods and services enables economic growth between members—Black queer men trading skills, services, and creative work within community, building wealth and reducing dependence on exploitative labour markets. Mental health first aid training adapted for Black queer men's experiences, supporting 200 men/year to become better friends to each other—recognising signs of distress, offering compassionate support, and building community care capacity without professionalised gatekeeping. Community organiser training builds capacity for democratic participation and collective action, ensuring community power extends beyond this programme into broader organizing.
Service gap bridging fund enables fellows to respond to urgent needs they identify—therapy subsidies before breakdown, housing deposits before street homelessness, crisis support before suicide attempt. Democratic allocation through community governance, not institutional gatekeeping.
Legal advice and financial literacy: Fellows embedded in legal advocacy and employment sectors provide access to immigration support, housing rights, employment law, and financial planning. Addressing how economic precarity and legal vulnerability compound mental health crisis, recognising financial precarity as trauma rather than personal failure.
Recognising internal diversity: Black queer men are not a homogeneous group. Family therapy development supports parents navigating relationships with their sons, particularly where families struggle with religious conservatism, migration trauma, or intergenerational cultural differences. Relationship counselling addresses intimate partner dynamics, helping men build healthy relationships whilst navigating racism and homophobia's effects on connection and trust. Later life care ensures older Black queer men—particularly those who survived 1980s-90s HIV crisis, police violence, and Section 28—receive dignity, connection, and culturally competent support as they age. These interventions recognise that mental health operates across life stages, family systems, and intimate relationships, not just in isolated individuals.
Responding to Powerlessness: Democratic Infrastructure
BLKOUT's Community Benefit Society extends into deliberative democracy infrastructure. Years 1-2: Fellows report learning to community governance. Year 3: Community decides infrastructure priorities for Years 6-10 (housing? media? archive? care co-op?). Years 4-5: Development lab coordinates from deliberation through piloting. Platform connects fellows, community, and democratic participation. Community evaluation ensures accountability: Are fellows creating change or being tokenised? Are relationships transforming outcomes?
Emergency response and contingency funds enable adaptation to unanticipated crises. Full financial detail, including all budget lines and reparative justice connections, available in the Cost Model paper.
This IS the UN reparations framework in practice:
- Restitution: Fellowship programme restoring Black queer men to sector leadership positions colonialism and racism denied
- Compensation: Career investment, professional development, cross-sector experience (vs. unpaid community labour + workplace victimisation)
- Rehabilitation: Cohort model + consultancy advocacy healing Black workers from sector employment practices that isolate and harm, building collective power to resist institutional violence
- Satisfaction: Fellows visibly leading reform whilst community democratically directs resources and infrastructure
- Guarantees of non-repetition: Fellows become future sector leaders and consultancy team, building institutional capacity to limit racism and homophobia's power over Black queer workers, transformation compounds intergenerationally
The Return on Investment
Investing in Black queer men as sector leaders generates returns across careers, communities, and systems:
Career transformation for 10 Black queer men creates sector leadership cohort. Each specialist gains 5 years professional development, institutional reform expertise, and career acceleration. By Year 5, they're positioned as directors, senior managers, policy leads across mental health, housing, and social care. Their career trajectories shift from isolated, victimised workers to championed sector leaders. This is reparations: restoring Black queer men to positions colonialism denied.
Institutional systems change through cohort leadership. Ten specialists reforming NHS pathways, housing practices, and social care approaches affect thousands beyond the 35,000 Black queer men directly served. Unlike isolated Black workers whose efforts institutions ignore, the cohort's collective power + consultancy team backing makes their insights undeniable. Institutions either transform or lose access to specialist expertise community provides.
Prevented crisis costs through specialist-identified interventions. Each suicide prevented saves £3.12M. Each psychiatric admission avoided saves £10,000+. Each homelessness emergency placement prevented saves £73,000/year. The service gap bridging fund (£1.2M) enables specialists to prevent crises they see coming—therapy subsidies before breakdown, housing deposits before street homelessness, crisis support before suicide attempt.
Community capacity beyond mental health. Digital platform connecting 35,000 people + democratic governance infrastructure create organising capacity. The cohort of specialists become community champions—not just in their day jobs, but as leaders mobilizing for broader change. Infrastructure decided Years 3-5 delivers in Years 6-10: community land trust? Media co-op? Archive? Social care cooperative? Whatever community decides, specialists lead delivery.
Knowledge generation for sector-wide reform. The cohort documents what works in co-producing services with communities. Their learning transfers to other marginalised populations, other sectors, other geographies. By Year 5, they're training other organisations, speaking at conferences, writing policy. The model scales: if 10 specialists transform 6 sectors in 5 years, imagine 100 specialists across 20 sectors in 10 years.
Account: Creating Accountability for Change
Why Past Institutional Failures Matter
Black queer men have every reason to distrust institutions that promise reform. The NHS has failed to address racism in mental health services despite decades of evidence. LGBTQ+ organisations have centred white experiences whilst marginalising Black voices. Local authorities have consulted communities without acting on what they learn.
Accountability for past failures isn't about blame; it's about establishing conditions for future trust. When institutions acknowledge that their services haven't worked for Black queer communities, they create foundation for genuine partnership. Without that acknowledgment, communities reasonably ask: why would we expect different outcomes this time?
Partnership Requires Shared Accountability
Community oversight ensures that services funded through this investment remain community-controlled. Governance boards with majority community representation, transparent decision-making about resource allocation, and community veto power over major changes prevent drift back to institutional control.
Outcome measurement defined by communities tracks what actually matters. Reduction in suicidal ideation, increased community connection, restoration of cultural practices, and economic participation replace narrow clinical metrics that miss broader wellbeing.
Institutional learning treats community-led innovation as expertise that can inform mainstream services. When peer support outperforms professional services, the response isn't to absorb successful community programmes into NHS bureaucracy—it's for NHS to learn from different approaches to service design and delivery.
Ongoing investment recognises that one-time funding doesn't create sustainability. Initial £95 million infrastructure investment requires follow-on funding for operations, maintenance, and evolution. Accountability means committing to partnership beyond pilot phases and demonstration projects.
The Offer to Be Better
This investment offers government, business, and civil society institutions opportunity to demonstrate genuine commitment to reform.
For government, this is chance to pioneer co-produced public services that deliver better outcomes at lower costs. Success with Black queer men's mental health creates blueprint for reforming services across health, housing, criminal justice, and education.
For business, this is opportunity to invest in communities as partners rather than markets. Corporate mental health spending often goes to workplace counselling services with limited effectiveness. Investment in community infrastructure that addresses structural causes of poor mental health delivers greater impact whilst building relationships with communities companies claim to support.
For civil society organisations, this is invitation to follow community leadership rather than assuming institutional expertise. Foundations and charities that fund community-defined priorities create more sustainable impact than grants that impose external agendas.
From Rhetoric to Action
While international debates about reparations continue between nations and across populations, we have immediate opportunity to demonstrate reparative justice in practice. The UN framework identifies what repair requires; this investment shows how to deliver it not through elite rhetoric in New York or Geneva in a generation's time, but through Black queer men leading mental health reform in NHS trusts and housing associations, supported cohort learning protecting them from workplace victimisation, and democratic governance ensuring community power from Greenwich to Glasgow, Bradford to Brixton, Swansea to Sunderland today.
The £10.5 million investment detailed in this briefing isn't abstract principle—it's career investment in Black queer men as sector leaders. Ten specialists with institutional placements, professional development, and cohort support. Consultancy team championing their success, not extracting their labour. Deliberative democracy infrastructure enabling 35,000 people to decide what gets built based on specialists' learning. Not predetermined solutions imposed on communities, not isolated tokens institutions victimise, but supported Black queer leaders transforming sectors with community governance backing.
This is social innovation from the margins showing public services how to reform with citizens rather than to them. Communities forged in the crucibles of difference develop solutions that institutions trained in the master's tools cannot imagine.
The choice before decision-makers is between expensive failure and cost-effective transformation. Current approaches generate high spending with low returns, managing symptoms whilst leaving causes untouched, responding to crises communities could prevent with proper support.
More fundamentally, the choice is between perpetuating systems that harm and partnering with communities to heal. Accountability for past institutional failures creates foundation for future trust. Acknowledgment that existing services haven't worked for Black queer communities opens space for trying approaches that do. Investment in community ownership rather than institutional control demonstrates commitment to genuine reform.
This briefing presents three accounts: describing reality of community innovation, counting real costs of investing in Black queer sector leaders, and establishing accountability frameworks ensuring specialists thrive rather than suffer workplace victimisation. All three converge on same conclusion: reparations means investing in Black queer men's careers, protecting them through cohort support, and ensuring their leadership transforms sectors whilst community governance decides what infrastructure emerges.
The account must be settled—described truthfully (Black workers currently isolated and victimised despite expertise), counted accurately (£10.5M investing in 10 specialists + cohort support + democratic governance), and made accountable collectively (community decides infrastructure, not institutions; specialists champion community priorities, not institutional extraction). Black queer men are ready for sector leadership. The question is whether institutions are ready to invest in our success rather than benefit from our failure.